- Catalogs
- Agappe Diagnostics Switzerland GmbH
- KL-6 Mispa i60 CLEIA
KL-6 Mispa i60 CLEIA
1 /1Page
KL-6 Mispa i60 CLEIA
1 /1Page
Catalog excerpts

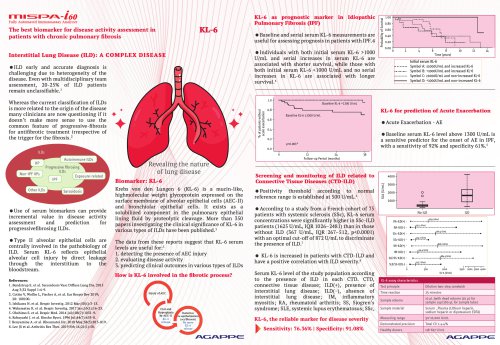
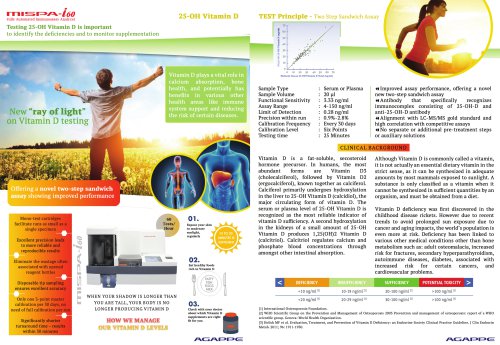
Fully Automated Immunoassay Analyzer The best biomarker for disease activity assessment in patients with chronic pulmonary fibrosis KL-6 Interstitial Lung Disease (ILD): A COMPLEX DISEASE • ILD early and accurate diagnosis is challenging due to heterogeneity of the disease. Even with multidisciplinary team assessment, 20-25% of ILD patients remain unclassifiable.1 Whereas the current classification of ILDs is more related to the origin of the disease many clinicians are now questioning if it doesn’t make more sense to use the common feature of progressive-fibrosis for antifibrotic treatment irrespective of the trigger for the fibrosis.2 KL-6 as prognostic marker in Idiopathic Pulmonary Fibrosis (IPF) • Baseline and serial serum KL-6 measurements are useful for assessing prognosis in patients with IPF.4 • Individuals with both initial serum KL-6 >1000 U/mL and serial increases in serum KL-6 are associated with shorter survival, while those with both initial serum KL-6 <1000 U/mL and no serial increases in KL-6 are associated with longer survival.4 Symbol A: >ioooU/mL and increased KL-6 Symbol B: <l000U/mLand increased KL-6 Symbol C: >l000U/mL and non-increased KL-6 Symbol D: <ioooU/mL and non-increased KL-6 KL-6 for prediction of Acute Exacerbation• Acute Exacerbation - AE • Baseline serum KL-6 level above 1300 U/mL is a sensitive predictor for the onset of AE in IPF, with a sensitivity of 92% and specificity 61%.5 • Use of serum biomarkers can provide incremental value in disease activity assessment and prediction for progressivefibrosing ILDs. • Type II alveolar epithelial cells are centrally involved in the pathobiology of ILD. Serum KL-6 reflects epithelial alveolar cell injury by direct leakage through the interstitium to the bloodstream. 1. Bendstrup E. et al. Sarcoidosis Vase Diffuse Lung Dis. 2015 Aug 3;32 Suppl 1:4-9. 2. Cottin V, Wollin L, Fischer A, et al. Eur Respir Rev 2019; 3. Ishikawa N. et al. Respir Investig. 2012 Mar;50(l):3-13. 4. Wakamatsu K. et al. Respir Investig. 2017 Jan;55(l):16-23. 6. Kobayashi J. et al. Rinsho Byori. 1996 Jul;44(7):653-8. Revealing the nature of lung disease Biomarker: KL-6 Krebs von den Lungen 6 (KL-6) is a mucin-like, highmolecular weight glycoprotein expressed on the surface membrane of alveolar epithelial cells (AEC-II) and bronchiolar epithelial cells. It exists as a solubilized component in the pulmonary epithelial lining fluid by proteolytic cleavage. More than 350 papers investigating the clinical significance of KL-6 in various types of ILDs have been published.3 The data from these reports suggest that KL-6 serum levels are useful for:3 1. detecting the presence of AEC injury 2. evaluating disease activity 3. predicting clinical outcomes in various types of ILDs How is KL-6 involved in the fibrotic process? Screening and monitoring of ILD related to Connective Tissue Diseases (CTD-ILD) • Positivity threshold according to normal reference range is established at 500 U/mL.6 • According to a study from a French cohort of 75 patients with systemic sclerosis (SSc), KL-6 serum concentrations were significantly higher in SSc-ILD patients (1625 U/mL, IOR 1026-2481) than in those without ILD (367 U/mL, IOR 267-512, p<0.0001) with an optimal cut-off of 872 U/mL to discriminate the presence of ILD.7 • KL-6 is increased in patients with CTD-ILD and have a positive correlation with ILD severity.8 Serum KL-6 level of the study population according to the presence of ILD in each CTD. CTD, connective tissue disease; ILD(+), presence of interstitial lung disease; ILD(-), absence of interstitial lung disease; IM, inflammatory myositis; RA, rheumatoid arthritis; SS, Sjogren’s syndrome; SLE, systemic lupus erythematosus; SSc, KL-6, the reliable marker for disease severity ^ Sensitivity: 76.36% | Specificity: 91.08%
Open the catalog to page 1All Agappe Diagnostics Switzerland GmbH catalogs and technical brochures
 Mispa CXL Pro
Mispa CXL Pro2 Pages
 Mispa plus
Mispa plus2 Pages
 mispa i3
mispa i32 Pages
 Product List
Product List52 Pages

Archived catalogs
 Mispa Clog +
Mispa Clog +2 Pages
 Mispa CX4
Mispa CX411 Pages
 Mispa i4
Mispa i42 Pages
 Mispa Label
Mispa Label2 Pages
 Mispa i2
Mispa i22 Pages
 Corporate Brochure
Corporate Brochure60 Pages
 Mispa Count
Mispa Count2 Pages
 AGAPPE LIPIDS
AGAPPE LIPIDS8 Pages
 Mispa CountX
Mispa CountX2 Pages
 Mispa Count Plus - 5 part
Mispa Count Plus - 5 part2 Pages
 Mispa VIVA
Mispa VIVA2 Pages
- Molecular biology reagent
- AGAPPE laboratory reagent
- Diagnostic reagent
- Protein reagent
- Clinical chemistry reagent kit
- AGAPPE biochemistry analyzer
- Quality control reagent
- Immunoanalysis reagent kit
- Bacteria reagent
- AGAPPE automatic biochemistry analyzer
- AGAPPE benchtop biochemistry analyzer
- Blood sample reagent
- AGAPPE hematology analyzer
- AGAPPE automatic hematology analyzer
- Freeze-dried reagent kit
- PCR system
- AGAPPE benchtop hematology analyzer
- Automated immunoassay analyzer
- Clinical diagnostic immunoassay analyzer