Group: Olympus

Catalog excerpts

TECHNICAL INFORMATION SHEET MINIMALLY INVASIVE SURGERY TECHNICAL INFORMATION SHEET MINIMALLY INVASIVE SURGERY HALLUX VALGUS POST-OPERATIVE MANAGEMENT Document produced by the GRECMIP group (Research and Study Group for Minimally Invasive Foot Surgery) and the TALUS group from GECO (www.geco-medical.org) - 2005. In vast majority of cases, surgery can be performed on an out-patient basis: - with the patient returning home the same day, - with a surgical shoe with a stiff sole which is worn for 1 to 3 weeks. Minimally invasive treatment for Hallux Valgus should meet the same criteria as open surgery and should allow one: Full weight-bearing is allowed from the start, but it is important to organise rest periods with the foot elevated. 1. to realign the first phalanx on the M1 head, 2. to reduce DMAA angle, > The patient is seen again on day 8: - the dressing is removed, - non-absorbable sutures can be removed. - a silicon orthotic spacer is made by the surgeon or podiatrist. This is worn for a maximum of 2 weeks. Radiographic follow-up is then performed with the spacer in position. The patient leaves with a transverse metatarsal arch, which is supported by a cohesive elastic bandage. 3. to reduce the medial prominence of the head, 4. to release the lateral portion of the metatarsophalangeal joint of the 1st ray and to release its adductor, Result after 8 days with the spacer in place 5. to incorporate a varus osteotomy of the base of P1. The standard technique does not include fixation of metatarsal and phalangeal osteotomies, which are held in the corrected position by the post-operative dressing in the first week, by an orthosis (spacer) in the following two or three weeks. > The patient re-attends after one month for a second radiographic and clinical assessment, this time performed under loading and without the spacer ; the post-operative shoe having been replaced two weeks earlier by a flexible sports type shoe. 6 months post-operative view, showing a correction by minimally invasive surgery > The patient attends again between three to four months for final radiographic and clinical assessment. The timing of later follow-up varies, but is generally performed annually. MINIMALLY INVASIVE SURGERY Fiches A4 chirug mini-inva 4P GB This technique cannot be performed without specific instrumentation. This surgery is only indicated for a primary congenital deformity without arthrosis, where the 1st metatarso-phalangeal articulation is congruent (pathological DMAA angle > 7°) and the varus metatarsal angle is less than or equal to 16°. Radiographic follow-up at 8 days PATIENT POSITIONING POUR UNE GESTION FACILE BLOC OPERATOIRE OPTIONAL ASSOCIATED PROCEEDURES Because an image intensifier must be used to monitor osseous procedures and adjust osteotomies, the patient needs to be positioned as follows: - in the strict dorsal decubitus position, - with the operated foot extending beyond the edge of the table, - with the opposite foot on a support with the knee bent. > 2, 3 or even 4 recession osteotomies of the metatarsal heads: EQUIPMENT: - handle for Beaver surgical knife - ref. 254 327 / Beaver blade - ref. 248 435 - Shannon Recta burr 2.0 x 12 mm - ref. 256 018 - elevator - ref. 253 937 > Multiple tenotomies and capsulotomies of the lesser toes: EQUIPMENT: - handle for Beaver surgical knife - ref. 254 327 / Beaver blade - ref. 248 435 Additional proceedures on the lateral rays of the foot and/or lesser toes can be performed using similar techniques, such as: The fluoroscope is positioned at the side of the operated foot. Positioning of the patient and use of mini-fluoroscope (Mini C arm) > Multiple osteotomies of the lesser toes: EQUIPMENT: - Shannon Corta burr 2.0 x 08 mm - ref. 256 019 - handle for Beaver surgical knife - ref. 254 327 / Beaver blade - ref. 248 435 - elevator - ref. 253 937 Conception/creation: 1 ST STEP: REDUCTION OF THE MEDIAL PROMINENCE OF THE HEAD AND THE REVERDIN-ISHAM OSTEOTOMY Using a Beaver surgical knife (handle for Beaver surgical knife - ref. 254 327 / Beaver blade - ref. 248 435), make an incision antero medial to the M1 head directed towards the medial eminence.
Open the catalog to page 1
Fiches A4 chirug mini-inva 4P GB TECHNICAL INFORMATION SHEET FIRST STEP (CONTINUED) 3RD STEP: THE AKIN PHALANGEAL OSTEOTOMY Using a “windshield wiper” action in contact with the bone creates a working space, which can be expanded by using an elevator (Elevator - ref. 253 937). Wedge burr is placed into contact with the bone and makes it possible to shave, step by step, the medial part of the head. The burr is selected according to bone quality and the extent of the desired metatarsal correction. (Wedge burr 3.1 x 13 mm - ref. 256 016 or Wedge burr 4.1 x 13 mm - ref. 256 017). Using a third...
Open the catalog to page 2All FH Orthopedics catalogs and technical brochures
-
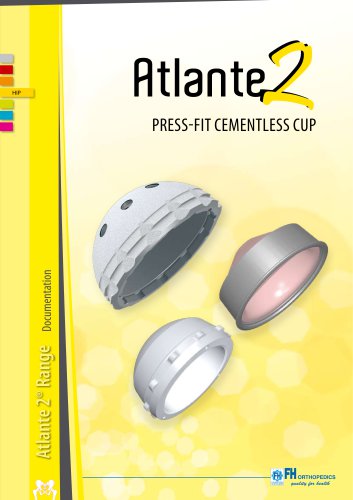
 CEMENTLESS PRESS-FIT CUP
CEMENTLESS PRESS-FIT CUP4 Pages
-
 Tenolig documentation
Tenolig documentation2 Pages
-
 TYLOS
TYLOS8 Pages
-
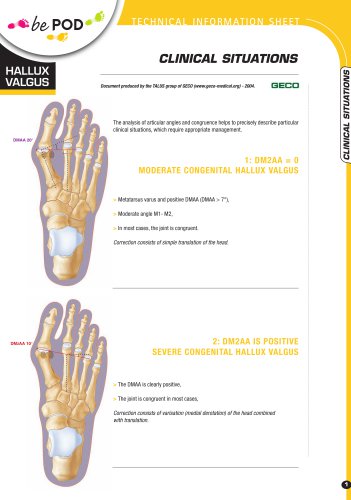
 PHALANGEAL OSTEOTOMY
PHALANGEAL OSTEOTOMY2 Pages
-
 MIS burs
MIS burs3 Pages
-
 Self-compressive screw
Self-compressive screw3 Pages
-
 Forefoot operative technique
Forefoot operative technique2 Pages
-
 FHK
FHK4 Pages
-
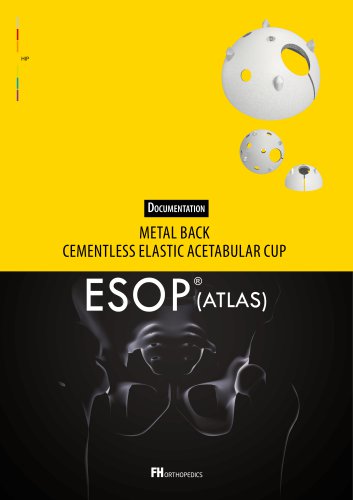
 ESOP (Atlante 2)
ESOP (Atlante 2)4 Pages
-
 Hip'n go stem
Hip'n go stem4 Pages