- Catalogs
- OPELAIII Cx
- Case Study N°3 Effectiveness of OPELAIII in Breast Surgery
- Company
- Products
- Catalogs
- News & Trends
- Exhibitions
Case Study N°3 Effectiveness of OPELAIII in Breast Surgery

Case Study N°3 Effectiveness of OPELAIII in Breast Surgery
This document discusses the effectiveness of the OPELAⅢ lighting system in surgical procedures, particularly in breast oncology surgeries. The focus is on its ability to illuminate deep and narrow surgical fields, enhancing visibility and aiding in precise surgical operations.
Surgical Case Overview
The document presents a case of mastectomy where a tumor was located in the upper-outer part of the left breast. The surgical field required a 15 cm incision. As the surgery progressed, deeper tissue flaps formed, necessitating enhanced lighting, which was effectively provided by OPELAⅢ.
Specifications and Features of OPELAⅢ
OPELAⅢ is highlighted for its ability to illuminate deep surgical fields, even with narrow incisions. This feature is particularly beneficial in maintaining esthetic outcomes post-surgery. The system allows for clear visibility of nerves, blood vessels, and adipose tissues, reducing the risk of surgical errors.
Procedures and Applications
OPELAⅢ is especially useful in axillary lymph node dissection, where it provides sufficient light to distinguish critical anatomical structures. The document emphasizes its role in breast reconstruction surgeries, where precise identification of internal mammary artery perforators is crucial.
Recommendations and Future Prospects
The document suggests the potential for further enhancements, such as voice activation for light adjustments, to improve surgical efficiency. OPELAⅢ's ability to provide targeted illumination without frequent adjustments is praised, making it suitable for complex procedures like axillary lymph node dissection.
Conclusion
OPELAⅢ is presented as a valuable tool in surgical settings, offering significant advantages in terms of visibility and precision. Its application in breast surgeries demonstrates its potential to improve surgical outcomes and patient safety.
Catalog excerpts

Dr. Seigo Nakamura Professor, Division of Breast Surgical Oncology, Department of Surgery, Showa University School of Medicine Open surgery in recent years in the field of breast oncology has increasingly shifted towards small incision even in deep areas because of the emphasis not only on minimal invasiveness but also on more esthetically favorable outcome. This time, we have asked Dr. Seigo Nakamura from the Division of Breast Surgical Oncology at Showa University to evaluate the effectivity of OPELAⅢ in open surgery of the breast, wherein the postoperative visual esthetic is always considered important. The brightness of OPELAⅢ penetrates even a deep and narrow surgical field This was a case of mastectomy where a tumor about 2 cm was palpated at upper-outer part of the left breast and was diagnosed as cancer after a biopsy. The surgical field was an incision of about 15 cm in length. The flesh closer to the incision could be dissected with relative ease, but as the surgery progressed deeper flaps of tissue began to form. And when the surgical field reached the depth near the end of the breast, OR light alone was no longer sufficient. It was then that OPELAⅢ showed its effectiveness in supplementing the light environment (Fig. 1). To inflate the breast back to its natural form after mastectomy, it would be ideal to leave as much normal skin as possible, which meant that the flaps need to be larger, essentially making the surgical field deeper and narrower. However, due to its ability to illuminate the depths even with narrow incision, OPELAⅢ overcame this antinomy, demonstrating its usefulness especially from an esthetic standpoint. Fig. 1Deep muscle tissue/ blood vessel can be recognized even when the large flap is formed OPELAⅢ is useful in axillary lymph node dissection as it illuminates exactly where I want to see In this surgery, the sentinel l ym p h n o d e w a s j u s t b e l o w t h e intercostobrachial nerve, which was another reason requiring deep incision (Fig. 2 and 3). Also, the subsequent axillary lymph node dissection was carried out while having to peer into a depth of 15 to 20 cm as the patient was rather overweight. It is extremely challenging to illuminate deep into the axilla with only the OR light. Even when the angle and focus are adjusted properly Fig. 2 eep inside where the sentinel lymph node used to be D ON means when OPELAⅢ is lit. sentinel lymph node used to be It can be clearly identified that the intercostobrachial nerve runs laterally as the surgery progresses
Open the catalog to page 1
at first, the area I want to see keeps changing as I separate the surrounding tissues during operation. So, the angle and focus needs to be adjusted repeatedly. There are retractors with lights on the tip, but they do not always illuminate where I really want to see. The advantage of using OPELAM is that the surgeon can adjust the light to illuminate exactly where he/she wants to see at will. I would say it is particularly suitable for procedures such as axillary lymph node dissection. The axilla contains the intercostobrachial nerve. Damaging it may result in paralysis of the upper arm. When...
Open the catalog to page 2All OPELAIII Cx catalogs and technical brochures
 OPELAⅢの有用性vol10市中病院編
OPELAⅢの有用性vol10市中病院編2 Pages
 OPELAⅢの有用性vol9美容外科領域
OPELAⅢの有用性vol9美容外科領域2 Pages
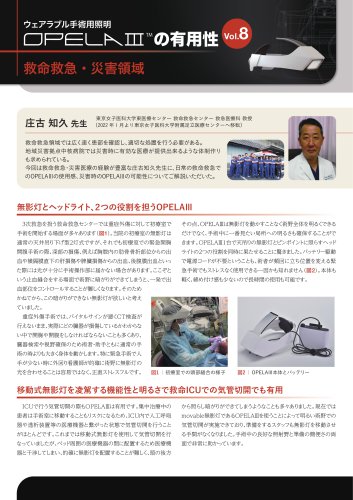 OPELAⅢの有用性vol8救命救急・災害領域
OPELAⅢの有用性vol8救命救急・災害領域2 Pages
 OPELAⅢの有用性vol7形成外科領域
OPELAⅢの有用性vol7形成外科領域2 Pages
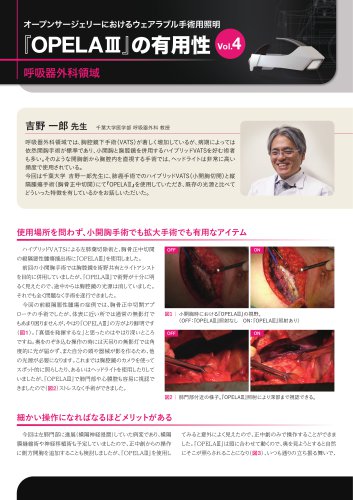 OPELAⅢの有用性vol4呼吸器外科領域
OPELAⅢの有用性vol4呼吸器外科領域2 Pages
 OPELAⅢの有用性vol3乳腺外科領域
OPELAⅢの有用性vol3乳腺外科領域2 Pages
 OPELAⅢの有用性vol2内分泌外科領域
OPELAⅢの有用性vol2内分泌外科領域2 Pages
 OPELAⅢの有用性vol1消化器外科領域
OPELAⅢの有用性vol1消化器外科領域2 Pages
 OPELAIII Instructions Manual
OPELAIII Instructions Manual32 Pages
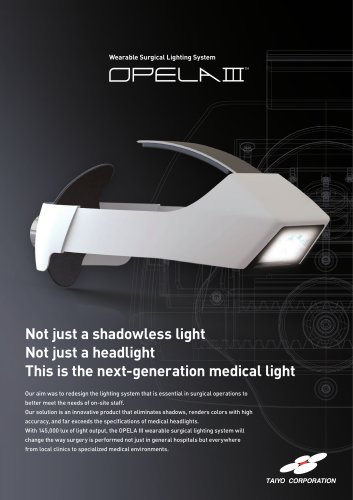 OPELAⅢ_Catalog_EN
OPELAⅢ_Catalog_EN2 Pages
 OPELAIII Cx Instructions Manual
OPELAIII Cx Instructions Manual48 Pages










