- Catalogs
- OPELAIII Cx
- Case Study N°4 Effectiveness of OPELAIII in Thoracic Surgery
- Company
- Products
- Catalogs
- News & Trends
- Exhibitions
Case Study N°4 Effectiveness of OPELAIII in Thoracic Surgery

Case Study N°4 Effectiveness of OPELAIII in Thoracic Surgery
This document discusses the use of OPELAⅢ, a lighting device, in thoracic surgery, specifically during hybrid VATS lobectomy and mediastinal malignant tumorectomy. Dr. Ichiro Yoshino from Chiba University shares his experiences and insights on the effectiveness of OPELAⅢ compared to conventional lighting methods.
Specifications and Features
OPELAⅢ is highlighted for its ability to provide ample lighting in surgical fields, even in deep cavities where traditional OR lights and thoracoscopes fall short. It is equipped with three LEDs, offering high light intensity and reducing shadows cast by the surgeon's hands and instruments.
Procedures and Applications
During surgeries, OPELAⅢ was used to enhance visibility, allowing the surgeon to turn off other light sources like the thoracoscope. It proved beneficial in both minor thoracotomy and extended surgeries, such as median sternotomy for tumor removal. The device's ability to direct light according to the surgeon's head movements improved the visibility of critical areas like the hilar and pericardial spaces.
Benefits and Recommendations
OPELAⅢ significantly reduced surgery time by improving visibility and reducing the need for additional lighting adjustments. It allowed for faster and more precise movements, minimizing stress and enhancing safety. The device is recommended for procedures requiring high precision due to its ability to illuminate deep surgical fields effectively.
Conclusion
OPELAⅢ is praised for its brightness and utility in thoracic surgeries, offering various intangible benefits beyond its primary function. It is considered a valuable tool for enhancing surgical precision and efficiency.
Catalog excerpts

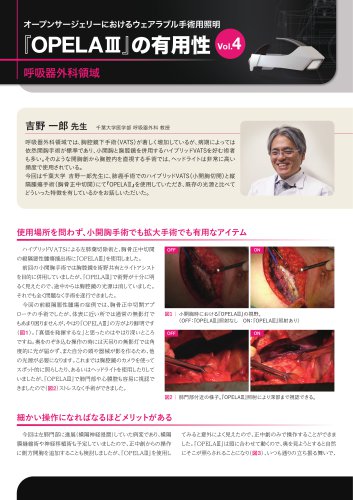
Dr. Ichiro Yoshino Professor, Department of Thoracic Surgery, Graduate School of Medicine, Chiba University In the field of thoracic surgery, video-assisted thoracic surgery (VATS) has markedly increased, but open thoracotomy remains the standard practice depending on the stage of the disease, and many surgeons prefer hybrid VATS with minor thoracotomy and thoracoscopy combined. Headlights are used very frequently in such open surgery which requires examining inside the thoracic cavity directly with one’ eyes. s This time, Dr. Ichiro Yoshino of Chiba University shared with us about the beneficial features of OPELAⅢ as compared with conventional light sources in lung cancer surgery through hybrid VATS (minor thoracotomy) and mediastinal tumor surgery (median sternotomy). Regardless of area, it is effective in both minor thoracotomy and extended surgery I used OPELAⅢ during a hybrid VATS lobectomy of left lung and mediastinal malignant tumorectomy through median sternotomy. Initially, I was using a thoracoscope in conjunction with OPELAⅢ to provide ample light in the surgical field. However, during operation it became apparent that the light from OPELAⅢ alone was more than enough therefore I chose to turn off the light of the thoracoscope, and had no problem completing the surgery. To remove the anterior mediastinal malignant tumor, a median sternotomy approach was taken. While OR lights usually provide sufficient brightness in the shallow region, using OPELAⅢ together proved to enhance visibility vividly (Fig. 1). I was most impressed with OPELAⅢ when it came to illuminating deep cavities. Normally, when looking down into deep areas, we need the help of another light source because the OR light on the ceiling cannot reach the depths or the surgeon’s head and instruments cast shadows over the surgical field. Until now we were using headlights or the camera on thoracoscopes to light up certain spots, but with OPELAⅢ, we performed the surgery with hardly any stress because it allowed us to easily recognize visually the hilar area as well as the pericardial space (Fig. 2). Fig. 1 he view with/without OPELAⅢ during small thoracotomy T ON means when OPELAⅢ is lit. Fig. 2The view near the hilar area. It is visible into the depths with OPELAⅢ. ON means when OPELAⅢ is lit. OPELAⅢ becomes even more beneficial when the procedure demands greater precision I was initially thinking of performing lateral thoracotomy in addition to median sternotomy because a diaphragm plication and nerve grafting were necessary as the lesion was extended to the left hilar area (phrenic nerve invasion). However, OPELAⅢ provided exceptional visibility beyond expectation therefore eventually only median sternotomy was sufficient. This was achieved because OPELAⅢ can point the light in the direction of my head’s movement, illuminating where I want to see even into the depths (Fig. 3), and improving visibility of the surgica
Open the catalog to page 1
Wearable Surgical Lighting System in Open Surgery VoM Thoracic Surgery Everything I wanted to see this time looked bright. I think the more precision the procedure requires, the more benefit you can get out of it. OPELAM is certainly an item I would continue to use for additional value on safety. Fig. 3 I Scene from the surgery using OPELAM. By illuminating from various angles, light can be directed deep into surgical fields where OR light cannot reach. My hands and instruments cast less shadows, so the field of view remains brightly illuminated I have always used headlights during thoracotomy...
Open the catalog to page 2All OPELAIII Cx catalogs and technical brochures
 OPELAⅢの有用性vol10市中病院編
OPELAⅢの有用性vol10市中病院編2 Pages
 OPELAⅢの有用性vol9美容外科領域
OPELAⅢの有用性vol9美容外科領域2 Pages
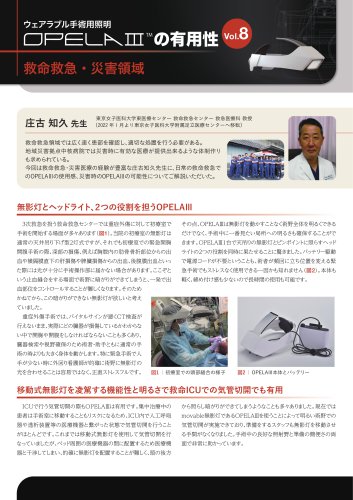 OPELAⅢの有用性vol8救命救急・災害領域
OPELAⅢの有用性vol8救命救急・災害領域2 Pages
 OPELAⅢの有用性vol7形成外科領域
OPELAⅢの有用性vol7形成外科領域2 Pages
 OPELAⅢの有用性vol4呼吸器外科領域
OPELAⅢの有用性vol4呼吸器外科領域2 Pages
 OPELAⅢの有用性vol3乳腺外科領域
OPELAⅢの有用性vol3乳腺外科領域2 Pages
 OPELAⅢの有用性vol2内分泌外科領域
OPELAⅢの有用性vol2内分泌外科領域2 Pages
 OPELAⅢの有用性vol1消化器外科領域
OPELAⅢの有用性vol1消化器外科領域2 Pages
 OPELAIII Instructions Manual
OPELAIII Instructions Manual32 Pages
 OPELAⅢ_Catalog_EN
OPELAⅢ_Catalog_EN2 Pages
 OPELAIII Cx Instructions Manual
OPELAIII Cx Instructions Manual48 Pages










