FreeO2-Emergency-ERS-2015
FreeO2-Emergency-ERS-2015
Oxygen therapy is a critical component in emergency and critical care settings, but its administration is often dependent on staff workload. The study introduces FreeO2, a device designed to automate oxygen titration to maintain target SpO2 levels, potentially reducing staff workload and improving compliance with oxygen administration guidelines.
Methods
This multicentric international randomized controlled study compared the FreeO2 device with manual oxygen adjustment in patients admitted to the emergency department for acute respiratory failure (ARF) requiring oxygen therapy of at least 3L/min. Patients were randomized to receive either automated or manual oxygen adjustment for three hours, with continuous SpO2 monitoring.
Results
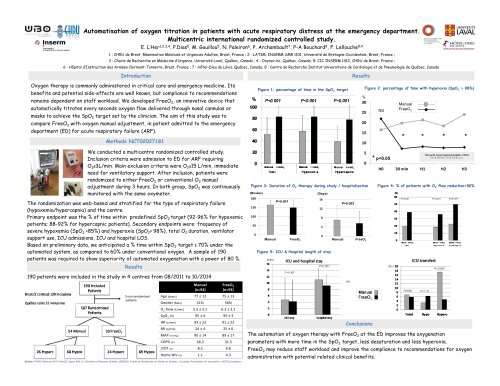
The study included 190 patients across four centers. The primary endpoint was the percentage of time within the predefined SpO2 target (92-96% for hypoxemic patients; 88-92% for hypercapnic patients). Secondary endpoints included the frequency of severe hypoxemia and hyperoxia, total oxygen duration, ventilator support use, ICU admissions, and length of stay in ICU and hospital. The FreeO2 group showed improved oxygenation parameters, with more time spent within the SpO2 target range, less desaturation, and less hyperoxia compared to the manual group. The study anticipated a 70% time within the SpO2 target for the automated system, compared to 60% for conventional oxygen.
Conclusions
Automated oxygen therapy with FreeO2 in the emergency department improves oxygenation parameters and may reduce staff workload, enhancing compliance with oxygen administration recommendations and potentially offering clinical benefits.
Figures and Data
Figures in the study illustrated the percentage of time in the SpO2 target, time with hyperoxia, duration of oxygen therapy, and percentage of patients with significant oxygen flow reduction. The data showed significant improvements in the FreeO2 group compared to the manual group.
Funding
The study was funded by PHRC National 2010 FreeO2 Hypox #08-12, the Ministry of Finances Québec, Fonds de Recherche en Santé du Québec, Canadian Foundation for Innovation, and IUCPQ foundation.
Catalog excerpts

Automatisation of oxygen titration in patients with acute respiratory distress at the emergency department. Multicentric international randomized controlled study. E. L’Her1,2,3,4, P.Dias5, M. Gouillou5, N. Paleiron6, P. Archambault7, P-A Bouchard8, F. Lellouche8,4 1 : CHRU de Brest, Réanimation Médicale et Urgences Adultes, Brest, France ; 2 : LATIM, INSERM UMR 1101, Université de Bretagne Occidentale, Brest, France ; 3 : Chaire de Recherche en Médecine d’Urgence, Université Laval, Québec, Canada ; 4 : Oxynov.inc, Québec, Canada; 5: CIC INSERM 1412, CHRU de Brest, France ; 6 : Hôpital d’Instruction des Armées Clermont-Tonnerre, Brest, France ; 7 : Hôtel-Dieu de Lévis, Québec, Canada; 8 : Centre de Recherche Institut Universitaire de Cardiologie et de Pneumologie de Québec, Canada Oxygen therapy is commonly administered in critical care and emergency medicine. Its Figure 1: percentage of time in the SpO2 target benefits and potential side-effects are well known, but compliance to recommendations Figure 2: percentage of time with hyperoxia (SpO2 > 98%) remains dependent on staff workload. We developed FreeO2, an innovative device that automatically titrates every seconds oxygen flow delivered through nasal cannulas or masks to achieve the SpO2 target set by the clinician. The aim of this study was to compare FreeO2 with oxygen manual adjustment, in patient admitted to the emergency department (ED) for acute respiratory failure (ARF). We conducted a multicentre randomized controlled study. Inclusion criteria were admission to ED for ARF requiring O2≥3L/min. Main exclusion criteria were O2≥15 L/min, immediate need for ventilatory support. After inclusion, patients were randomized to either FreeO2 or conventional O2 manual adjustment during 3 hours. In both group, SpO2 was continuously monitored with the same oxymeter. The randomization was web-based and stratified for the type of respiratory failure (hypoxemia/hypercapnia) and the centre. Primary endpoint was the % of time within predefined SpO2 target (92-96% for hypoxemic patients; 88-92% for hypercapnic patients). Secondary endpoints were: frequency of severe hypoxemia (SpO2 <85%) and hyperoxia (SpO2> 98%), total O2 duration, ventilator support use, ICU admissions, ICU and hospital LOS. Based on preliminary data, we anticipated a % time within SpO2 target ≥ 70% under the automated system, as compared to 60% under conventional oxygen. A sample of 190 patients was required to show superiority of automated oxygenation with a power of 80 %. Figure 3: Duration of O2 therapy during study / hospitalization (Minutes) Figure 4: % of patients with O2 flow reduction>50% Figure 5: ICU & Hospital length of stay Results 190 patients were included in the study in 4 centres from 08/2011 to 10/2014 Manual (n=94) 3 non randomized patients Grants: PHRC National 2010 FreeO2 Hypox #08-12, Ministery of finances Québec (MDEIE), Fonds de Recherche en Santé du Québec, Canadian Foundation for Innovation, IUCPQ foundation Conclusions The automation of oxygen therapy with FreeO2 at the ED improves the oxygenation parameters with more time in the SpO2 target, less desaturation and less hyperoxia. FreeO2 may reduce staff workload and improve the compliance to recommendations
Open the catalog to page 1All OxyNov catalogs and technical brochures
 FreeO2-Rehab-CRC-2011
FreeO2-Rehab-CRC-20112 Pages
